HQIP-Commissioned Audit Sees 72.8% Increase in School Healthcare Plans for Young People with Epilepsy
17 Sep 2025
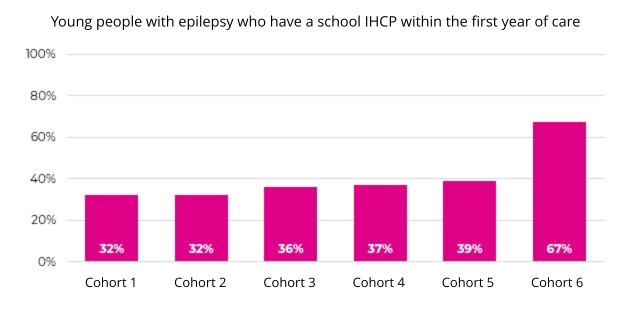
The proportion of children and young people with epilepsy who have a school Individual Healthcare Plan (IHCP) within the first year of care has jumped 72.8%, from 38.9% in the 2024 annual report to 67.2% in the latest Epilepsy12 audit 2025 report. This marked increase, after previously being broadly static for several years, highlights a major step forward in ensuring that children with epilepsy receive the support they need in school.
Epilepsy12, the national clinical audit of seizures and epilepsies in children and young people, is commissioned by HQIP as part of the National Clinical Audit and Patient Outcomes Programme (NCAPOP) and has tracked paediatric epilepsy care since 2009 across England and Wales. Delivered by the Royal College of Paediatrics and Child Health (RCPCH), the audit provides essential data to benchmark services against national standards, and drive improvements and reduce variation in care.
A key factor behind the increased proportion of children and young people with IHCPs has been the direct involvement of children, young people and families themselves. The Epilepsy12 Youth Advocates group, who are epilepsy experienced or interested young people and families volunteering to improve care for patients, has been instrumental in shaping what is measured, helping to define Epilepsy 12’s key performance indicators and highlighting the issues and potential solutions.
This brings patient-led priorities to the audit, ensuring that topics such as school care plans and the mental health of children and young people with epilepsies are central, alongside more traditional healthcare metrics. This shift in focus, and the resulting improvements at scale, is a major success for the young people driving and benefitting from the improvements.
The Importance of School Healthcare Plans
IHCPs have been a key focus for the Youth Advocates (YAs) and other stakeholders over the last few years. The YAs have consistently emphasised that a good, individualised plan in school can be transformative, especially in the first year after diagnosis. Having an IHCP is key to ensuring that children and young people with epilepsy receive appropriate support, safety, and full participation in education and school life. They are vital for epilepsy, as what is right for one child can be completely different from what is right for another.
The YAs emphasised the importance of IHCPs and how they can support not only the young person, but also their family, teachers and friends to feel more confident about epilepsy. They also advocated for a comprehensive epilepsy IHCP template for schools that included crucial information, including seizure details, aspirations, and mental health, but was also easy to use. An example template was developed and is available online.
“I was diagnosed with epilepsy in 2018. My parents and I met with the School Nurse and Headmaster to create a plan. Teachers were informed and updates were made as needed. It was a learning curve for everyone. The plan allowed me to attend day trips, complete two Duke of Edinburgh’s expeditions, and go on a 7-night trip to America. Without this support, travelling would have been much more difficult.” A young person with epilepsy
Looking forward: Opportunities for further improvements
Given that having an IHCP is a statutory requirement for a young person with epilepsy, Epilepsy12 is aiming for 100% adoption and identifying easier ways to enable the sharing of key information between families, health and education. As well as continuing to build upon existing successful work to improve this KPI, encouraging further data entry and service participation will also be important. There have been significant increases in the total cohort size of health service providers submitting data to the audit and of data completeness this year, something which is extremely important when drawing conclusions from the audit data; particularly trends over time and variation between subgroups.
150 NHS Health Boards and Trusts providing paediatric epilepsy care in England and Wales were registered into the Epilepsy12 audit in 2025, via a bespoke data platform launched in December 2023. This is an increase from the 138 Health Boards and Trusts registered to the platform used previously. Of the Health Boards and Trusts registered, 80% (120/150) submitted data in this latest round of reporting (cohort 6, covering children and young people with a first paediatric assessment undertaken between 1 December 2022 and 30 November 2023).
The cohort size also increased considerably, with 3,105 young people with newly-diagnosed epilepsy included in the 2025 analysis. This compares to the previous five cohorts, which all had around 2,000 young people. Furthermore, data completeness has improved from 86% in cohort 5 (2024 report) to 98.5% in cohort 6 (2025 report).
The increased cohort size and improved data completeness may be a reflection of the streamlined data entry process on the new Epilepsy12 data platform. Find out more about this and other highlights, including epilepsy specialist nurse provision improvements, in the 2025 Epilepsy12 report.
Going forward, as well as striving to further improve data entry and service participation, the focus of the audit will continue to be reviewed. Indeed, Epilepsy12 has often seen the ambition for a particular KPI advance over time, building upon initial progress by resetting aspirations and targets. This means that the current KPI focused upon young people with epilepsy having a school care plan may well evolve – for example to having a ‘comprehensive’ IHCP and then an ‘impactful’ plan.
Epilepsy12’s latest findings underscore the importance not only of robust data, but also the power of involving children and young people in shaping the care that directly impacts their lives. By embedding patient and family at the heart of its work, it has demonstrated how genuine collaboration and co-production can deliver real-world change.
These noteworthy improvements in paediatric epilepsy care reflect not only robust national audit and patient-led advocacy, but also the ongoing commitment of key stakeholders. Initiatives such as the NHS England Epilepsy Oversight Group, including the publication of the national bundle of care for children and young people with epilepsy, and targeted programmes like the Epilepsy Quality Improvement Programme (EQIP) have driven up performance and consistency.
Furthermore, the collaborative efforts of key stakeholder groups, including Young Epilepsy, Epilepsy Action and others, ensure that the needs of children, young people, and families remain central, embedding best practice and delivering meaningful change.
Having an effective individual school healthcare plan is a vital step towards safer, equitable and empowering support for young people with an epilepsy. Seeing such a dramatic improvement in schools shows what is possible when professionals, families and young people work together at many different levels.” Dr Colin Dunkley, Clinical Lead for Epilepsy12
Further information and resources
- Epilepsy12 2025 report
- Interview with Epilepsy12 on what effective patient engagement means in practice
- More about the Epilepsy12 audit, with previous reports
- A guide to patient and public involvement in quality improvement
- E-learning: Introduction to quality improvement for patients and public
- Epilepsy12 Audit case study – how patients and carers influence the production of patient-focused outputs from the programme

Other news

Benchmarking data published
Data relating to epilepsy has been published on HQIP's benchmarking site, NCAB.

New reports published
NEW RESOURCES to support improvement in healthcare, from HQIP's audits and programmes, have been published.

Benchmarking data published
Data relating to paediatric diabetes and perinatal mortality has been published on HQIP's benchmarking site, NCAB.













 These results weren’t achieved through heroic effort or top-down compliance. They came from:
These results weren’t achieved through heroic effort or top-down compliance. They came from: