Blog: Yes we can
24 Jun 2024
The importance of national clinical audit in addressing health inequalities
Professor Danny Keenan, Medical Director, HQIP
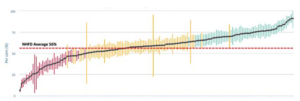
We all know instinctively that health inequalities are complex. Why a person who lives in an affluent area, or is white, is likely to have better health outcomes than their more deprived, or non-white, counterpart (for example) is difficult to unpick. But unpick it, we must. However, in doing this, we are not faced with a blank sheet of paper. We have data, which can support a better understanding of the issues and help us to tailor solutions. And that’s where national clinical audit comes in. For HQIP, as commissioner of the National Clinical Audit and Patient Outcomes Programme (NCAPOP) on behalf of NHS England, we understand the potential value of this vast font of knowledge (the NCAPOP is the largest of its type in the UK) in addressing health inequalities. In November 2023, we published a report on Improving Health Inequality Data in the NCAPOP, to explore the barriers to health inequality data being routinely reported within the programme. Written by our then-Medical Director’s Fellow, Dr Alice Bradley, this report found significant variations in the reporting, analysis, and use of health inequality data among different audits. Now that a little time has passed since this report was published, I want to reflect again on its findings, to ensure that the important messages within are kept to the fore and, more importantly, that the recommendations are implemented.This is a call to arms. We must utilise our collective initiative and resources to collect the data needed to enable insights in relation to ethnicity and deprivationThe report drew from two previous studies where we, with previous Fellows, looked at the outputs from a random group of NCAPOP audit reports, to identify which, if any, analyses were being performed in relation to the influence of ethnicity and deprivation on patient outcomes. Clearly, we were hoping to gain insights into any differing outcomes relating to these factors. However, we found there to be less focus on their influence than we had hoped. There was much good practice to support insights into the influence of gender and age – but much less in relation to deprivation, and even less, to ethnicity. Accordingly, we surveyed our audit providers to explore why this might be. From formal and informal discussions, we understood that they had much interest in understanding inequalities in relation to ethnicity and deprivation, but barriers persisted nonetheless. Alice piloted, and then undertook, a definitive survey to explore what these barriers might be. There was very good compliance in the survey from the audit providers, which supported a variety of findings. As might be expected, some issues are more easily solved than others. Therefore, it’s easier to consider them in terms of those that can be more easily overcome, alongside those that are more complex. Issues that can be more easily overcome can be summarised as follows:
- When using routine data sources:
- Poor or incomplete coding
- Difficulties with categorisation
- Miscoding, with different codes used for the same patient on different occasions.
- When using bespoke data:
- Time pressure on clinical staff
- Engagement challenges with patients
- Consent issues.
- Small numbers problem: At the analysis stage, this makes data analysis statistically inaccurate. Furthermore, there are concerns that small numbers at reporting stage may make data identifiable. There is currently a lack of guidance on how to aggregate small numbers.
- Population data: There is a lack of population statistics to allow comparisons to be made at the analysis stage.
- Costs: It was clear that detailed analysis along the lines of ethnicity and deprivation would increase the costs, increasing the resources required for clinical audits.
Data providers had much interest in understanding inequalities in relation to ethnicity and deprivation, but barriers persisted nonethelessA digital solution is the obvious approach to take. We must not rely on frontline staff working harder. The systems we use routinely must be used to solve this problem. With the significant roll-out of electronic records, there must be a way of incorporating information about ethnicity linked to NHS number, and about deprivation linked to postcode? And if this could be extended to linking between primary and secondary care, there would be even greater benefits. NHS Digital, now incorporated into NHS England, has already improved coding. This was a very important step that enables us to pick out, not just the ‘big picture’ differences in care and outcomes between different ethnic and socio-economic groups, but also the more nuanced differences. If we work together with agencies such as NHS England, the Welsh Government, the Model Health System, the UK Health Security Agency and the Office for Health Improvement and Disparities, we can move on to develop strategies to address more complex issues, such as the small numbers problem associated with health inequality data outlined above.
When faced with the COVID-19 pandemic, everyone came together to tackle difficult problems. The same approach is possible for health inequalitiesI want to end on a note of caution. Whatever strategies are developed, we must recognise that there will always be a population that is transitory or who want to remain private, for whatever reason. While difficult to include in national data collection, it is imperative that they are accommodated by whatever system we introduce to improve health inequalities. In summary, while there’s no denying that health inequalities are complex, appropriate data collection can help us to understand these complexities. As such, this blog is a call to arms. We must utilise our collective initiative and resources to gather the data needed to enable these insights to take place, particularly in relation to ethnicity and deprivation. Then we will be able to ‘blow the lid off’ health inequalities, and peer inside to understand why differences exist. More importantly, we can make changes to health and care – as well as other – services to transform and save many, many lives. I, for one, am ready for this challenge – and I know that the whole healthcare sector is too. Yes we can. This blog was released as part of Clinical Audit Awareness Week 2024; for more information, go to: www.hqip.org.uk/clinical-audit-awareness-week.
Further information
- The National Clinical Audit and Patient Outcomes Programme (NCAPOP)
- Report on Improving Health Inequality Data in the NCAPOP
- CORNERSTONE 2023, HQIP’s quality improvement magazine, with an article on health inequalities (pages 14-15)
- 2023 Clinical Audit Awareness Week / Clinical Audit Hero Healthcare Inequalities case study – Sandwell & West Birmingham NHS Trust
- Spotlight on the Early Years report to identify cross-cutting lessons relating to early years healthcare with a focus on health inequalities.
Other news

9 Jul 2026
New reports published
NEW RESOURCES to support improvement in healthcare, from HQIP's audits and programmes, have been published.

23 Jun 2026
CAAW26 Equity and Patient Involvement award winners announced
Find out who won the Equity and Patient Involvement category of the Excellence in Clinical Audit Awards 2026, part of Clinical Audit Awareness Week.

11 Jun 2026
New reports published
We are pleased to announce that the following NEW RESOURCES to support improvement in healthcare,...












 Trusts can either internally review these questions to judge where they might sit, or it may be helpful to ‘buddy’ with a peer Trust for independently reviewed opinions, such that a relevant professional team, external to the Trust / Board, provide ‘fresh eyes’ and an independent perspective. Translating national data into effective change at a local level isn’t easy. It may be littered with potential pitfalls and difficulties, but it is, of course, vitally important. So, I will leave you with just one takeaway thought, a lightbulb moment (neatly inspired by the inventor of the lightbulb, Thomas Edison): “I have not failed 700 times. I have succeeded in proving that those 700 ways will not work. When I have eliminated the ways that will not work, I will find the way that will work”. Here’s to continuing to work together, and supporting each other, to find the ‘right way’ to use national clinical data to support meaningful change at a local level.
Trusts can either internally review these questions to judge where they might sit, or it may be helpful to ‘buddy’ with a peer Trust for independently reviewed opinions, such that a relevant professional team, external to the Trust / Board, provide ‘fresh eyes’ and an independent perspective. Translating national data into effective change at a local level isn’t easy. It may be littered with potential pitfalls and difficulties, but it is, of course, vitally important. So, I will leave you with just one takeaway thought, a lightbulb moment (neatly inspired by the inventor of the lightbulb, Thomas Edison): “I have not failed 700 times. I have succeeded in proving that those 700 ways will not work. When I have eliminated the ways that will not work, I will find the way that will work”. Here’s to continuing to work together, and supporting each other, to find the ‘right way’ to use national clinical data to support meaningful change at a local level.