Avoiding ‘lost in translation’
Published: 05 Apr 2024
Using national healthcare data to support meaningful change
Jill Stoddart, Director of Operations (National Clinical Audit and Patient Outcome Programme), HQIP
What keeps you awake at night? When I worked in clinical practice, questioning whether I’d provided the very best care for patients kept me awake. Now I commission national clinical audits and other patient outcome programmes, this is still a primary concern – but the focus is on whether the data we collect supports the best care for patients. How can we ensure that evidence derived at a national level is well received and implemented at Trust level? And, critically, are we really making a difference to patient care?
I understand the pressure and challenges that Trusts face with increasing demand, financial constraints, bed shortages, recruitment freezes and preparing for winter pressures – all in addition to national and regional scrutiny. Against this backdrop, it can be extremely difficult to make sense, and practical use, of the vast array of national healthcare data available. Between April 2022 and March 2023, the National Clinical Audit and Patient Outcome Programme (NCAPOP), commissioned by HQIP, published 64 reports and 368 recommendations alone. Factor this up across the national clinical effectiveness landscape – including National Institute for Health and Care Excellence (NICE) guidance, Getting It Right First Time (GIRFT) reports, Healthcare Safety Investigation Branch (HSIB) investigations and multiple other national enquiries – and we can safely say that Trusts are awash with reports and recommendations.
Widely disseminate information about both negative and positive outliers – share the learning!
This is why, in 2023, HQIP reshaped its outputs. We undertook discussions with policy makers and healthcare providers, which identified a need to reduce the burden and increase the timeliness of data, culminating in:
- Shorter user-friendly ‘state of the nation’ reports
- Quality Improvement (QI) resources, replacing local recommendations in reports
- A focus on approximately ten metrics, and
- Near real-time dynamic reporting, refreshed at least quarterly.
However, while these changes were welcomed by healthcare providers, we know that information provision alone does not change behaviour. It takes much more than knowledge to leverage change. The starting point for transformation at a Trust level is to continually question the quality of care provided. Questions are vital, they do not mean resistance and should be actively encouraged. These questions can take many forms, and can help to clarify understanding.
Questions that healthcare organisations can ask themselves about their performance* were highlighted in the 2023 edition of CORNERSTONE by Mirek Skrypak (pages 22-23) and are worth reiterating here, since they are the starting point for a Trust:
- Do we know how good we are?
- Do we know where we stand relative to the best?
- Do we know where, and understand why, variation exists in our organisation?
- Over time, where are the gaps in our practice that indicate a need for change?
- In our efforts to improve, what’s working?
Alongside asking key questions about clinical effectiveness performance, all Trusts need to also invest time in building an open and transparent data and quality improvement culture. NHS England’s approach to improvement is outlined in their NHS IMPACT (Improving Patient Care Together) programme. It includes five components which form the ‘DNA’ of all evidence-based improvement methods, and which underpin a systematic approach to continuous improvement:
- Building a shared purpose and vision
- Investing in people and culture
- Developing leadership behaviours
- Building improvement capability and capacity, and
- Embedding improvement into management systems and processes.
NHS England also makes a wide variety of useful improvement resources available to health and other care providers. These include good practice pathways and guidance documents as well as cross-cutting workstreams such as GIRFT, intensive support and national clinical audit.
The starting point for innovation and change at a Trust level is to continually question the quality of care provide
So, what difference can clinical audit make? The audit cycle includes taking action to bring clinical practice in line with evidence based standards, to improve the quality of care and health outcomes. Healthcare providers need to consider the link between the evidence base, national policy, national clinical audit and local implementation. This can take many forms, but here are some top tips that are useful when considering how best to use data intelligently and achieve change at a local level:
- Share information widely across the Trust, understand variation, make data available and transparent but don’t stop there – discuss it and agree the changes required. Widely disseminate information about both negative and positive outliers – share the learning!
- Report by exception to the relevant assurance committees and Board – ensure regular Board airtime is given to discussing the data, its meaning and the required QI actions.
- Remove Trust level obstacles – bureaucracy stifles innovation.
- Remember the 80:20 rule (Pareto Principle) – 80% of outcomes (or outputs) result from 20% of causes (or inputs) for any given event.
- Always set deadlines and agree who is responsible for delivering actions, following up on progress. Set regular small milestones – these are much more likely to be successfully implemented.
- Action plans need to be robust and identify system actions which remove the reliance on individuals. Where possible, use standardised and permanent (physical or digital) designs to eliminate human error, sometimes referred to as ‘forcing actions’ (as cited in the Perinatal Mortality Review Tool (PMRT)’s infographic relating to their 2022 annual report).
- Be aware of national clinical audit publication schedules – and make plans to receive reports and data as they are published.
- Know your Trust plan and timetable for the national clinical audit programme.
- Monitor your own internal Trust data and take actions to unpick and explore early, using NHS England Making Data Count resources.
- Make an explicit Trust link between data and Quality Improvement (QI) and avoid silo working.
All seemingly obvious and sensible. But, in fact, it’s easy to get this wrong. The Kirkup report on maternity services at the East Kent University NHS FT was published in October 2022. It highlighted several important points when it comes to understanding variation, and presenting and interpreting data, stating “The unit-level information that is available tends to be presented in the form of ‘league tables’… These serve to conceal the variation between different units, with no indication of whether one or more units are outliers”. To address this, Kirkup noted two requirements:
1. From Section 6.9: The first [requirement] is the generation of measures that are:
- meaningful – that is, related clearly to outcomes
- risk adjustable
- available – they are available from data already routinely collected
- timely.
2. From Section 6.10: The second requirement is that the measures:
- are analysed and presented in a way that shows both random variation and trends
- use sound, statistically based approaches to detecting the signal among the noise
- are presented graphically to show variation, significant trends and outliers in the form of statistical process control charts and funnel
- plots are extended to clinically relevant outcome measures.
These, and many other messages in the Kirkup report, can be extrapolated and applied across Trusts and other healthcare providers. Data are everywhere, often difficult to interpret, can be complex and, at times, additional information is required to get a clear picture of what is happening. As such, it can be difficult for Trusts to understand where they need to improve. The following tools offer a suggested approach:
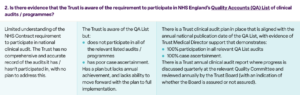
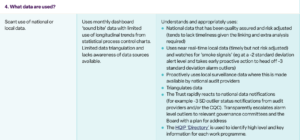
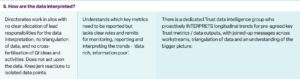
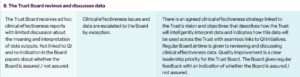
Questions for Trusts to ask themselves about how they use data



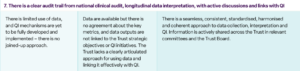
Trusts can either internally review these questions to judge where they might sit, or it may be helpful to ‘buddy’ with a peer Trust for independently reviewed opinions, such that a relevant professional team, external to the Trust / Board, provide ‘fresh eyes’ and an independent perspective. Translating national data into effective change at a local level isn’t easy. It may be littered with potential pitfalls and difficulties, but it is, of course, vitally important. So, I will leave you with just one takeaway thought, a lightbulb moment (neatly inspired by the inventor of the lightbulb, Thomas Edison): “I have not failed 700 times. I have succeeded in proving that those 700 ways will not work. When I have eliminated the ways that will not work, I will find the way that will work”. Here’s to continuing to work together, and supporting each other, to find the ‘right way’ to use national clinical data to support meaningful change at a local level.
Further information and resources
- HQIP commissioned audit and programme reports (subscribe to notifications here)
- Information and resources to support the use of the National Clinical Audit and Patient Outcome Programme (NCAPOP) to stimulate healthcare Quality Improvement (QI)
- Support with Developing a clinical audit programme
- NHS England Quality Accounts (QA) List of clinical audits/ programmes
- HQIP ‘Directory’ with high level and key information for each work programme
- National Clinical Audit Benchmarking (NCAB) website
- Article: When is data ‘good data’? HQIP CORNERSTONE magazine 2023 (pages 22-23)
- NHS IMPACT (IMproving PAtient Care Together) programme
- NHS England IMPACT resources and materials
- NHS England Making Data Count
This article was originally featured in HQIP’s quality improvement magazine, CORNERSTONE – to see more articles on topics such as healthcare inequalities and sustainability in healthcare, go to: www.hqip.org.uk/wp-content/uploads/2023/11/HQIP_Cornerstone_2024.pdf.